Crimean-Congo Hemorrhagic Fever (CCHF) in Pakistan: Emerging Threats, One Health Challenges, and Modern Control Strategies
Dr Muhammad Adil*
Technical Commercial Officer, Livestock Qaswa, DMG Pharmaceutical, Rawalpindi, Pakistan
Introduction
Crimean-Congo Hemorrhagic Fever is a severe emerging tick-borne zoonotic disease caused by the Crimean-Congo Hemorrhagic Fever Virus. The disease is endemic in Pakistan and several regions of Asia, Africa, the Middle East, and Eastern Europe. CCHF causes acute febrile illness, hemorrhagic manifestations, and multi-organ dysfunction, with reported case fatality rates ranging from 10–40%. Pakistan remains at high risk due to uncontrolled livestock movement, cross-border animal trade, inadequate tick control, climatic variability, and limited surveillance systems. High-risk groups include veterinarians, farmers, butchers, abattoir workers, and healthcare professionals. Strengthening integrated “One Health” strategies, including surveillance, vector control, biosafety, public awareness, and diagnostic capacity, is essential for effective prevention and outbreak management.
Etiology and Virology
Crimean-Congo Hemorrhagic Fever Virus (CCHFV), a member of the genus Orthonairovirus within the family Nairoviridae, is an enveloped, negative-sense single-stranded RNA virus possessing three genomic segments: Small (S), Medium (M), and Large (L). The virus demonstrates marked genetic diversity, with Asia-1 and Asia-2 genotypes reported in Pakistan. Due to its high pathogenicity and hemorrhagic potential, CCHFV requires Biosafety Level-4 (BSL-4) containment for viral isolation and propagation.
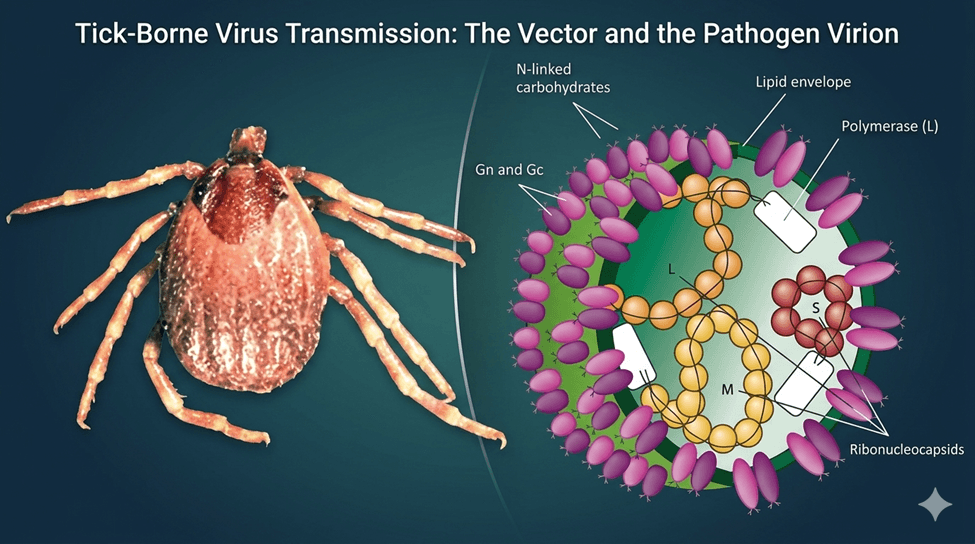
Fig.1: Hyalomma tick and CCHF virus morphology
Transmission:
The principal vector and reservoir of Crimean-Congo Hemorrhagic Fever Virus (CCHFV) is the hard tick of the genus Hyalomma. The virus is maintained in tick populations through transstadial and transovarial transmission, while horizontal transmission occurs among vertebrate hosts. Livestock including cattle, sheep, goats, and camels serve as important amplifying hosts, developing transient viremia without marked clinical signs and acting as silent reservoirs for zoonotic transmission to humans.
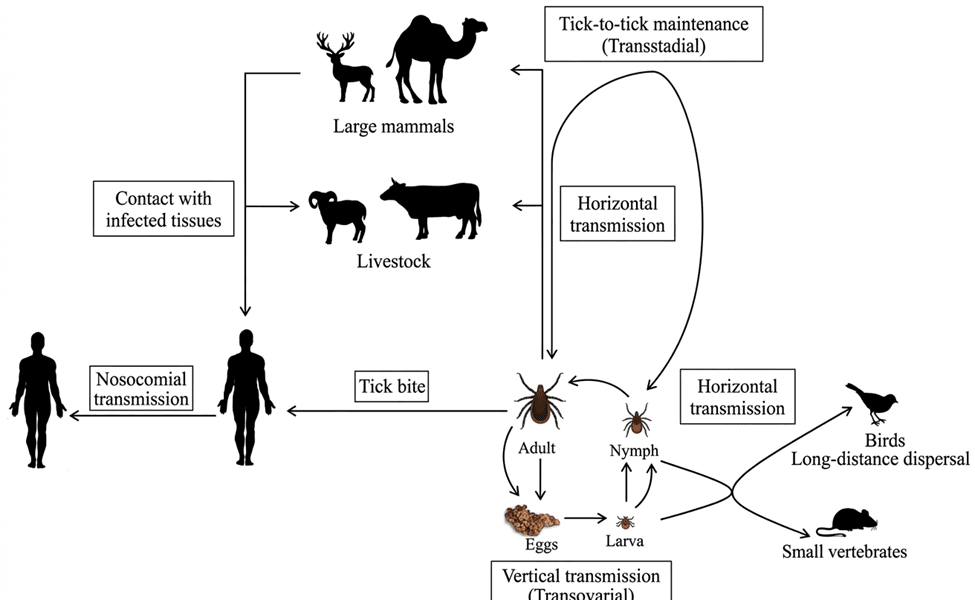
Fig.2: Mode of Transmission of CCHF
Epidemiology of CCHF in Pakistan
Pakistan reported its first confirmed case of Crimean-Congo Hemorrhagic Fever in 1976, and the disease is now endemic in Balochistan, Khyber Pakhtunkhwa, southern Punjab, and rural Sindh. Disease occurrence is strongly associated with seasonal tick activity, livestock movement, nomadic migration, inadequate veterinary surveillance, and poor slaughterhouse hygiene. Increased animal transportation during Eid al-Adha further elevates transmission risk.
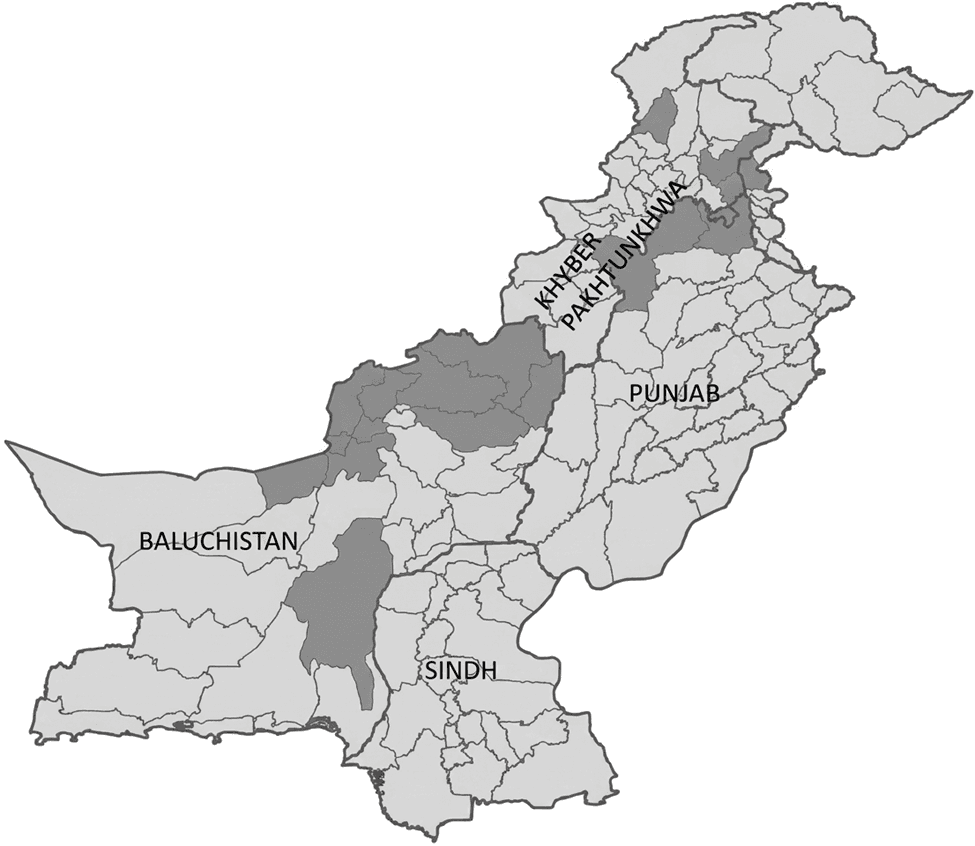
Fig.3: Geographic Distribution of Reported and Endemic Areas of Pakistan affected with CCHF
Border regions adjacent to Afghanistan remain highly vulnerable because of uncontrolled cross-border movement of livestock and tick-infested animals. Climatic factors, including rising temperatures, altered rainfall patterns, and prolonged warm seasons, also contribute to enhanced survival, reproduction, and geographic expansion of Hyalomma ticks, thereby facilitating CCHFV transmission.
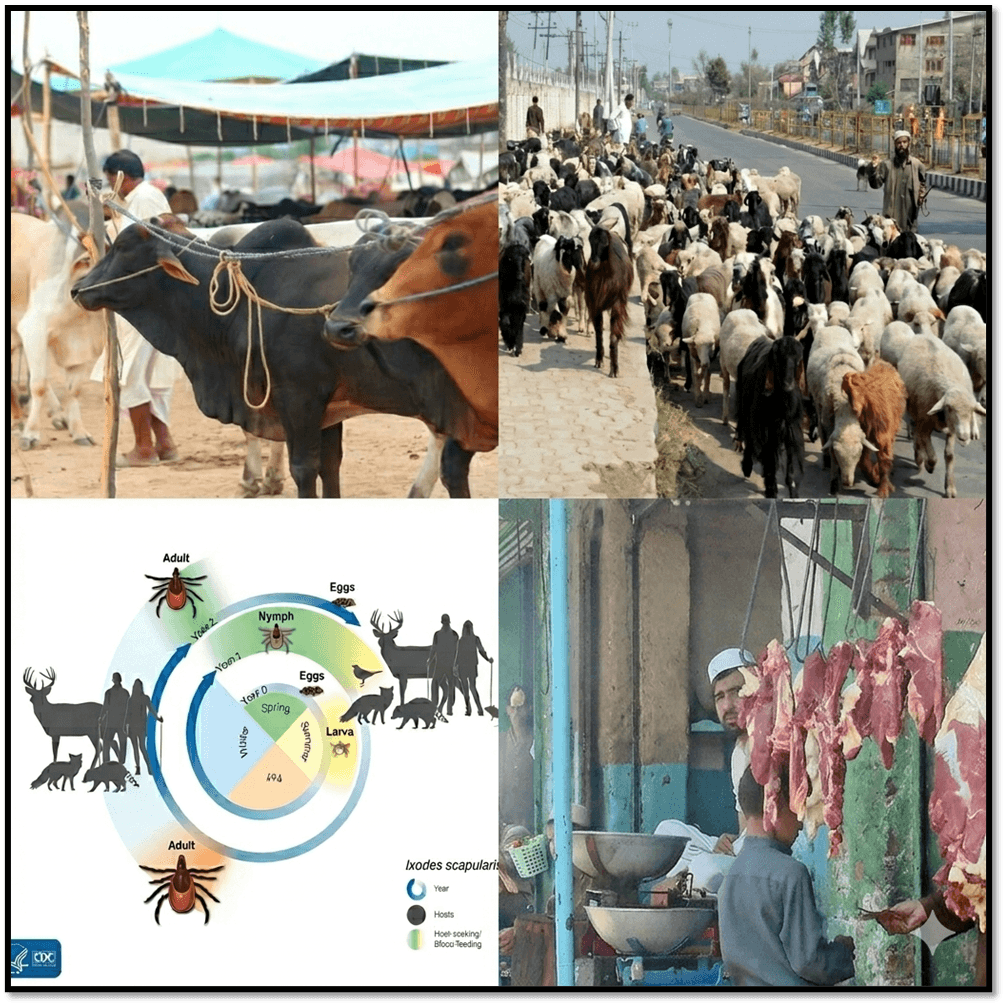
Fig.4: Role of climatic condition and uncontrolled movement of livestock across borders
Transmission Dynamics
Human infection with Crimean-Congo Hemorrhagic Fever Virus (CCHFV) occurs primarily through bites of infected Hyalomma ticks and direct contact with blood or tissues of viremic animals during slaughtering, veterinary procedures, meat processing, and animal parturition. Occupational groups at highest risk include farmers, veterinarians, abattoir workers, and livestock handlers. Nosocomial transmission also represents a major public health concern, occurring through exposure to infected blood, body fluids, contaminated needles, or aerosol-generating medical procedures, placing healthcare professionals at significant risk of hospital-associated outbreaks.
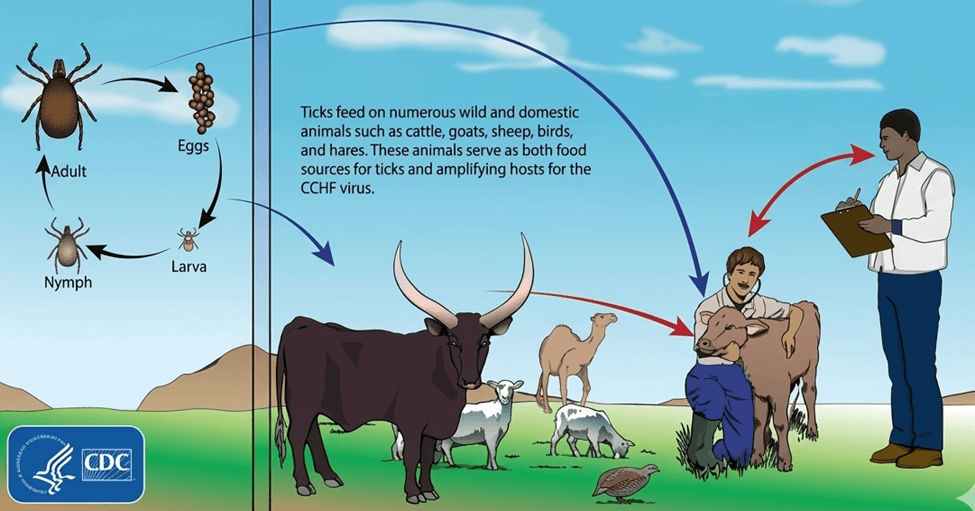
Fig.5: Transmission Dynamics and Host-to-Host Propagation
Pathogenesis and Clinical Manifestations
Following viral entry, Crimean-Congo Hemorrhagic Fever Virus (CCHFV) primarily infects endothelial cells, hepatocytes, monocytes/macrophages, and other immune cells, leading to endothelial injury and severe inflammatory responses. Excessive cytokine release, including TNF-α, IL-6, and interferons, contributes to increased vascular permeability, coagulation abnormalities, platelet consumption, hepatic injury, disseminated intravascular coagulation (DIC), hemorrhage, and multi-organ failure, which are associated with severe disease and poor prognosis.
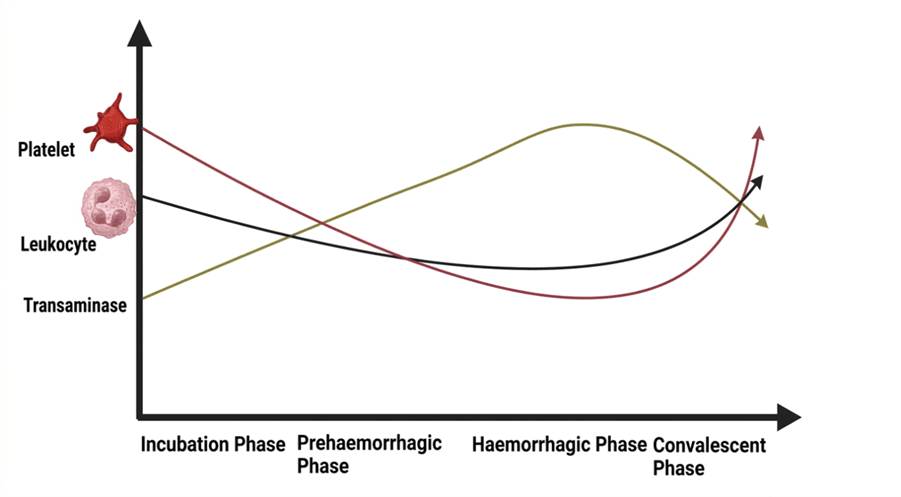
Fig.6: Dynamics in Hematology of different phases
Clinically, Crimean-Congo Hemorrhagic Fever progresses through incubation, pre-hemorrhagic, hemorrhagic, and convalescent phases. Early manifestations include sudden fever, headache, myalgia, gastrointestinal disturbances, and conjunctival congestion, followed by petechiae, epistaxis, hematemesis, hematuria, gingival bleeding, and shock in severe cases. During recovery, patients may experience prolonged weakness, tachycardia, neurocognitive disturbances, hair loss, mood alterations, and visual impairment.
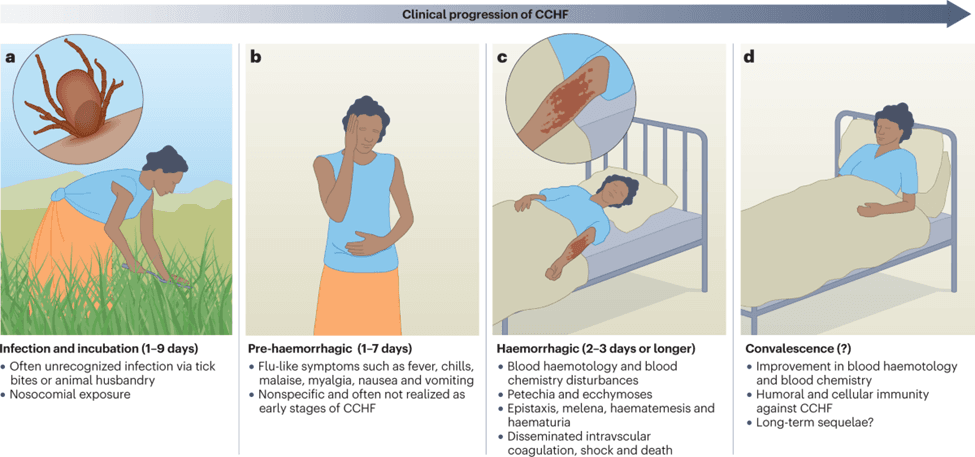
Fig.7: Clinical progression of CCHF in different phases
Laboratory Findings
Characteristic laboratory abnormalities in Crimean-Congo Hemorrhagic Fever include thrombocytopenia, leukopenia, elevated hepatic enzymes (AST, ALT), increased LDH and CPK levels, hyperbilirubinemia, prolonged PT/aPTT, and coagulation disturbances. Severe thrombocytopenia and marked elevation of liver enzymes are commonly associated with poor prognosis. Early diagnosis is essential for reducing mortality and controlling outbreaks, with Reverse Transcription Polymerase Chain Reaction (RT-PCR) considered the gold-standard diagnostic method due to its high sensitivity and specificity, while ELISA-based detection of IgM and IgG antibodies is widely used for identifying recent and past infections, respectively.
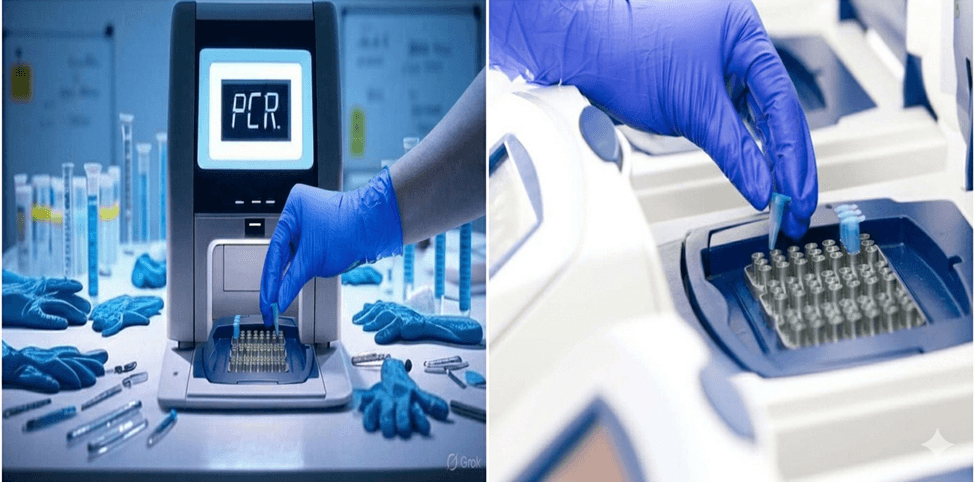
Fig.8: Technology for detecting CCHF
Treatment and Clinical Management
Currently, no specific approved antiviral therapy exists for Crimean-Congo Hemorrhagic Fever, and management is primarily supportive, including intravenous fluids, electrolyte correction, oxygen therapy, blood products (platelets, fresh frozen plasma), and hemodynamic stabilization. Ribavirin is the most commonly used antiviral agent, with better outcomes when administered early, although its clinical efficacy remains variable. Experimental options under investigation include favipiravir, monoclonal antibodies, interferon-based therapies, convalescent plasma, and RNA-targeted antiviral agents.
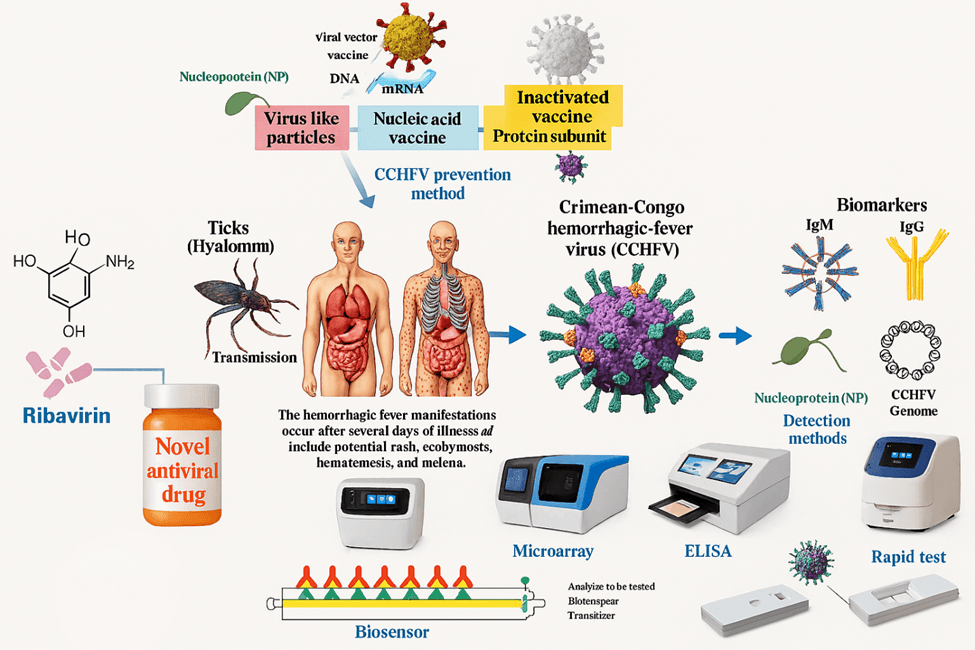
Fig.9: Novel treatment by using modern technology
One Health Perspective in CCHF Control
The One Health approach emphasizes the interdependence of human, animal, and environmental health in controlling Crimean-Congo Hemorrhagic Fever, as the virus persists within animal–tick ecosystems and cannot be effectively managed through isolated human-focused strategies. Effective prevention and control require multidisciplinary collaboration among veterinarians, physicians, epidemiologists, public health officials, wildlife experts, and environmental scientists, along with integrated surveillance systems to enable early detection and rapid response to outbreaks.
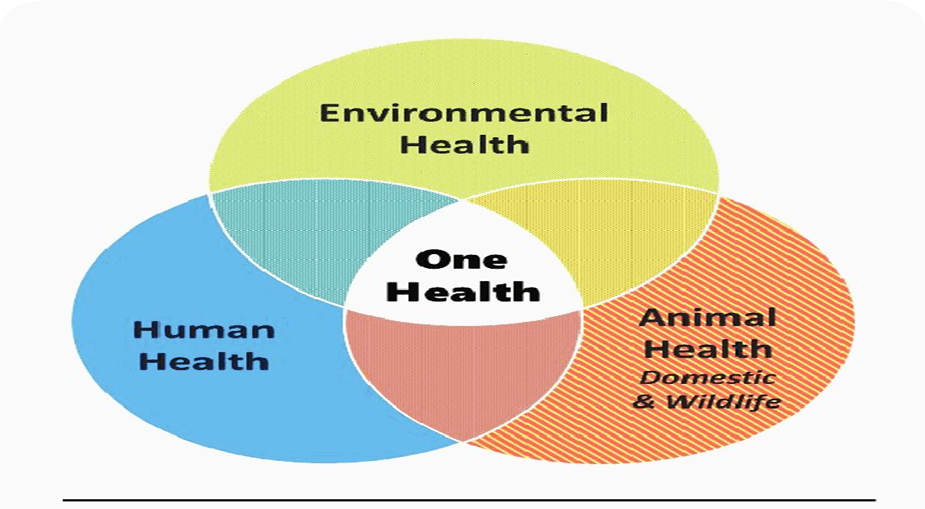
Fig.10: One Health Triad
Tick Ecology and Vector Control
Integrated tick management remains a critical strategy for preventing the transmission of Crimean-Congo Hemorrhagic Fever. Effective control measures include strategic acaricide application, rotational grazing, environmental sanitation, routine livestock inspection, and quarantine of newly introduced animals to reduce Hyalomma tick infestation and limit viral circulation among animal populations.
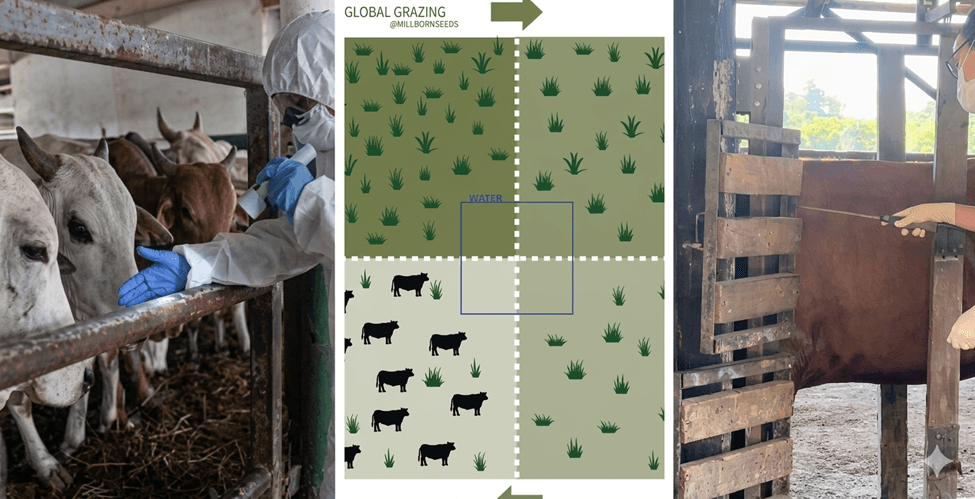
Fig.11: Quarantine, rotational grazing and acaricide application
Occupational Risk Groups
High-risk groups for Crimean-Congo Hemorrhagic Fever include veterinarians, farmers, slaughterhouse workers, healthcare personnel, and laboratory staff. Strict biosafety and infection-control measures are essential during animal handling and patient management, including isolation of suspected cases, appropriate personal protective equipment (PPE), barrier nursing, safe sharps disposal, controlled specimen handling, environmental disinfection, and contact tracing to minimize occupational and nosocomial transmission.
Recommendations for Pakistan
A coordinated national strategy is essential to reduce the burden of Crimean-Congo Hemorrhagic Fever in Pakistan, focusing on strengthening integrated One Health surveillance systems, expanding molecular diagnostic capacity, and establishing centralized outbreak databases. Effective tick control requires national acaricide management programs, integrated vector control strategies, and increased farmer awareness of tick ecology. Public health preparedness should include pre-Eid-ul-Adha awareness campaigns. Additionally, sustained research support, vaccine development, genomic surveillance, and interdisciplinary collaboration are critical for long-term disease control.
Conclusion
Crimean-Congo Hemorrhagic Fever remains an important zoonotic threat in Pakistan due to favorable ecological, climatic, and occupational factors supporting tick-borne transmission. Despite progress in diagnostics and supportive care, key gaps persist in surveillance, vector control, biosafety, and public awareness. Effective control depends on a strengthened One Health approach, improved veterinary–public health coordination, and sustained investment in research and outbreak preparedness at the national level.